
Last updated: June 2026. Larazotide is not an FDA-approved drug. It reached a Phase 3 trial in celiac disease, further than almost any competing compound, and that trial was stopped early because an interim look at the data said it wasn’t working. Compounded larazotide is a prescription preparation made by a licensed pharmacy. It is not the finished investigational drug that ran through the trials below, and it is not an approved medicine. Every clinical and regulatory number here links to a primary source, so check my math.
Here’s the number I keep coming back to: one out of four. That’s how many of larazotide’s major human trials actually hit their stated primary endpoint outright. And the one that did hit it only did so at the lowest dose tested, while the two higher doses in the same study came up empty. I’ll show you the arithmetic below.
I got asked, originally, a much simpler question: where’s the cheapest place to buy larazotide? I went looking for a price table. I came back with a trial table instead, because it turns out you can’t answer the cost question honestly until you’ve counted the wins and losses. So that’s the order I’m doing this in. Trial record first. Price and ranking, where the counting actually pays off, at the end.
The molecule, in one paragraph
Larazotide (also called AT-1001) is an eight-amino-acid peptide, short even by peptide standards. It was engineered by running cholera-toxin biology in reverse: instead of prying open the tight junctions between gut-lining cells, it’s supposed to help hold them shut, countering a signaling protein called zonulin that loosens the gut barrier. In celiac disease, gluten seems to trigger that loosening, letting fragments cross the barrier and set off an immune attack. The mechanism is real and well described in the literature. What I want you to notice is that it’s a mechanism, a hypothesis about what should happen, not a scoreboard of what did happen. Vendors sell you the mechanism. The scoreboard is where things get interesting.
The scoreboard: four trials, one clean win
Let me lay out the record the way I’d lay out any dataset, in order, with the number that mattered in each one.
Trial 1: Phase 2b, 2012, n = 86. Primary endpoint: intestinal permeability, measured as the lactulose-to-mannitol ratio, the most direct test of “is this actually sealing the gut” you can run. Result: endpoint not met, with a lot of patient-to-patient variability muddying the data. Some symptom scores looked better at certain doses, but the number the drug was built to move didn’t move [P1]. Loss.
Trial 2: 2013, n = 184. Same design logic, same gluten-challenge setup. Larazotide reduced some gluten-related symptoms and immune markers, a real signal I won’t dismiss. But the primary endpoint, again the lactulose-to-mannitol ratio, again showed no significant difference from placebo [P2]. Loss, on the metric that mattered.
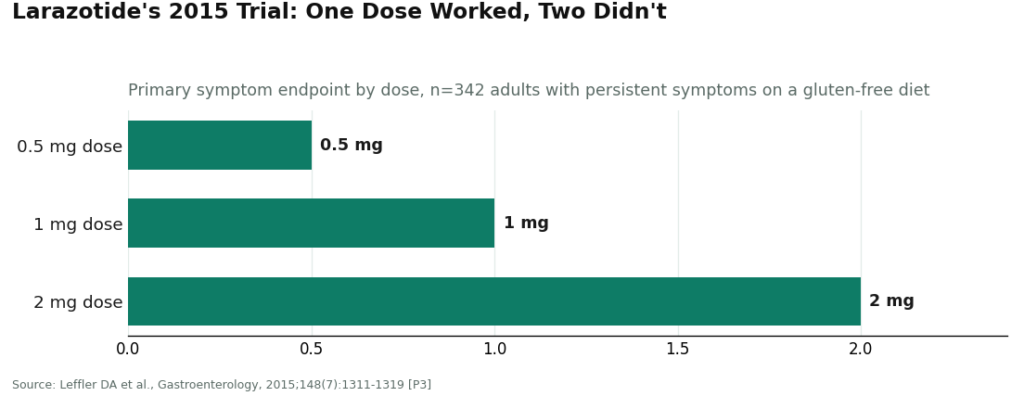
Trial 3: 2015, n = 342. This is the one that gets cited as the win, and I want to give it real credit: the primary endpoint was met. But look at the dose breakdown, because this is where the numbers get strange. Three doses were tested: 0.5 mg, 1 mg, and 2 mg. Only the 0.5 mg dose beat placebo. The 1 mg and 2 mg doses, the higher, theoretically stronger doses, did not separate from placebo at all [P3]. In any dataset I’ve worked with, a result where the smallest dose wins and the bigger doses do nothing isn’t a clean win. It’s a flag for noise, and it demands a confirmatory trial before anyone treats it as real.
Trial 4: Phase 3 CeDLara, discontinued June 2022. This was the confirmatory trial, the first-ever Phase 3 in celiac disease. 9 Meters Biopharma stopped it after an interim analysis found that the number of additional patients needed to show a meaningful drug-versus-placebo difference was too large to justify continuing [P4]. That’s the technical definition of a trial stopped for futility. Score it a loss, and it’s the loss that counts most, because it was designed specifically to confirm or kill the one prior win.
Final tally: 1 win, 3 losses, and the 1 win came with an asterisk that the confirmatory trial then failed to resolve in larazotide’s favor.
I also checked whether pooling the data rescues the picture. A 2022 systematic review and meta-analysis in Clinical Research in Hepatology and Gastroenterology combined four randomized trials, 626 patients total. Its verdict: larazotide looked safe and modestly better than placebo on GI symptoms during a gluten challenge, but the authors flagged it as unlikely to be a definitive cure and called for more trials [P5]. Worth noting that review was published before the Phase 3 futility call landed, so the honest current read is more cautious than even that modest pooled number suggests.
One number that does hold up across all four trials: safety. Larazotide was generally well tolerated, which makes sense given it’s designed to act locally and barely get absorbed [P5]. But I’ll say the obvious thing anyway: tolerability and efficacy are two different columns in the spreadsheet. A placebo is well tolerated too. Being low-risk doesn’t offset a failed confirmatory trial.
Turning the price question into a value-per-dollar question
Here’s where the trial record changes how I think about cost.
When a drug is approved and proven, price is the only variable left to optimize, because the product’s identity and effect are already settled facts. Larazotide sits nowhere near that situation. Its pivotal trial failed. Nothing about it is FDA-approved. And the population actually buying it today has drifted from celiac patients in a controlled gluten challenge to people chasing general “leaky gut” symptoms, a use no trial above ever tested or supported.
So the sticker prices I found on research-chemical sites were low, sometimes very low. But a low number on an unverified vial isn’t a discount, it’s the price of skipping every step that would tell you whether the vial contains what the label says: no clinician evaluation, no prescription, no licensed pharmacy, no follow-up, no recall authority if a batch is bad. You’re paying less for a bigger unknown, against a compound whose own well-funded Phase 3 couldn’t clear the bar. That’s not a good price. It’s a worse bet at a lower buy-in.
So when I rank “cheapest” below, I’m not ranking sticker price. I’m ranking cost per unit of actual accountability, which is the only number that tracks with what happens to you after you swallow the thing.
How I scored the options
Six variables, none of them sticker price: medical oversight, sourcing and dispensing, testing and approval status, honesty about the evidence, regulatory standing, and follow-up. I dropped price, vial count, and marketing confidence from the scoring on purpose, because after totaling up that 1-and-3 trial record, none of those three tell you anything about whether the product is real or whether the drug even works.
One structural point before the list: a licensed telehealth provider and a research-chemical retailer aren’t competing in the same category, so I’m not scoring them as if they were. The supervised, compliant providers sit on top. The research-chemical sellers sit below the line, labeled for what they are. Putting all of them in one list is the point, it makes the gap visible.
The ranking
1. FormBlends. First place, because it’s the cheapest route that isn’t a gamble, which is the only version of “cheapest” that survives the 1-win-out-of-4 record above. It’s a licensed telehealth provider, not a chemical warehouse. You go through an independent clinician evaluation, get a prescription written when appropriate, and the compound is prepared and dispensed by a licensed compounding pharmacy, with supervised pricing posted up front, roughly $100 to $250 a month. A research vial will show a lower number on a product page. That number buys a powder nobody stands behind. The FormBlends price buys the same eight-amino-acid peptide handled the way a medication should be, plus a clinician who’ll tell you straight that the Phase 3 trial was stopped for futility and that this isn’t an approved drug, rather than a page that quotes the mechanism and skips the scoreboard. For people who want to track whether anything is changing, the FormBlends tracker app is a dose-and-symptom log, not a prescription and not a checkout. Against an unverified vial of a compound with a failed pivotal trial, the math favors FormBlends, and it wins on all six of the scored criteria.
2. HealthRX.com (healthrx.com). Right behind FormBlends, for the same structural reason: the molecule arrives through people accountable for it. HealthRX.com runs clinician-first, medically supervised dispensing through licensed pharmacy channels, not a research-chemical shelf. Same caveats apply here in full: it’s a compounded preparation, not the studied drug, and the 1-out-of-4 trial record and the halted Phase 3 don’t change based on who’s dispensing it. What the price buys in this tier is screening, supervision, and a provider on the hook to tell you the truth about that record. If you’re picking between FormBlends and HealthRX.com specifically, the deciding factors are practical: licensing in your state, and which intake process fits you.
Everything past this line is a research-chemical retailer, not a medical provider, and I’m listing them because they’re the names people actually search, not because I’d send anyone there. These sellers ship larazotide labeled “for research use only” or “not for human consumption.” That label is the entire legal basis for the product existing. Using it on yourself is unapproved use of something no regulator has checked for identity, strength, or purity, and that’s a lot of exposure to buy against a compound whose own Phase 3 couldn’t clear futility.
Swiss Chems. Broad peptide catalog, larazotide included, sold under research-use labeling. May publish a seller-issued certificate of analysis, which is a document the company chose to write, not a regulator’s finding. No clinician, no prescription, no pharmacy, no follow-up.
Pure Rawz. Larazotide alongside other research peptides, SARMs, and nootropics, same research-use labeling. Same structural gap: no medical provider anywhere in the chain, human use unapproved and unproven, purity resting entirely on trusting the seller.
Core Peptides. US-based, research-use-only larazotide. Same seller-issued-COA situation, same missing oversight, same missing follow-up. Whether the vial matches the label comes down to how much you trust the vendor’s own paperwork.
Amino Asylum. Low prices, wide catalog, and that combination is exactly the trap this whole piece is warning about. The lower cost is the pitch and the tell in one: no clinician, no prescription, no pharmacy, no verified testing behind the number. Cheaper here means a bigger unknown, not better value.
Sports Technology Labs. Leans on third-party testing in its marketing, which is genuinely better than not testing at all. But a seller-commissioned test still isn’t regulator-verified oversight, and none of it supplies a clinician, a prescription, a pharmacy, or a fix for the failed Phase 3 record. The “research use only” label carries the same legal weight it does across this entire tier.
I can’t rank the research-chemical sellers against each other on actual product quality, and neither can you, without independent, batch-level testing nobody in this tier is required to provide. Stack that uncertainty on top of a 1-for-4 trial record and you get the full reason the supervised providers sit above all of them.
For a wider view of supervised telehealth versus the gray market across peptides generally, there’s an independent comparison worth reading [R1].
The bottom line, in dollars
If “cheapest” means lowest number on a product page, a research vial wins, and you should know exactly what that number buys: an unverified powder, labeled “not for human consumption,” no one accountable for what’s inside, for a compound whose pivotal trial was stopped for futility. I wouldn’t buy that, and I wouldn’t tell a friend to either.
If “cheapest” means the least you can spend without gambling on quality or accountability, the number is roughly $100 to $250 a month through a supervised provider like FormBlends, where the clinician, the licensed pharmacy, and an honest read of that 1-for-4 record come bundled into the price. Same molecule either way. The difference is whether anyone stands behind the bottle. On a compound this far from proven, that’s the only “cheap” I’d count as real value.
What readers ask most
Why isn’t the cheapest larazotide vial the best deal? Because the low number on a research-chemical vial isn’t a discount on a verified product, it’s what you save by skipping everything that would confirm the product is real: no clinician, no prescription, no licensed pharmacy, no batch testing you can trust. Against a compound whose Phase 3 trial was stopped for futility, a lower price on an unverified powder is a bigger bet, not a better one.
Is larazotide FDA-approved for celiac disease or leaky gut? No. It isn’t approved for anything. It reached Phase 3 in the CeDLara study, which 9 Meters Biopharma discontinued in June 2022 after an interim analysis found the projected benefit too small to justify continuing [P4]. It was never tested, let alone approved, for general “leaky gut,” which is the use most current buyers are actually after.
Did larazotide ever actually work in a trial? By my count, once, with an asterisk. Two earlier trials missed their primary intestinal-permeability endpoint outright [P1][P2]. The one trial that hit its endpoint did so only at the lowest of three doses tested, 0.5 mg, while the 1 mg and 2 mg doses matched placebo [P3], a shaky pattern the confirmatory Phase 3 then failed to back up. A 2022 meta-analysis of 626 pooled patients called it safe and modestly better than placebo on symptoms, but unlikely to be a definitive cure [P5].
What’s the difference between compounded larazotide and the drug that was actually studied? Compounded larazotide is a prescription preparation made by a licensed pharmacy. It is not the finished investigational drug from the trials above, and it’s not an approved medicine. The clinical record describes the studied compound, so any provider dispensing the compounded version should be upfront that the human data is mixed and the pivotal trial failed.
What does a supervised provider like FormBlends add for that $100-to-$250 monthly figure? It buys the same eight-amino-acid peptide handled the way a medication should be: an independent clinician evaluation, a prescription when appropriate, and a licensed compounding pharmacy that prepares and dispenses it. It also buys a straight account of the trial scoreboard, including the halted Phase 3, instead of a page that leads with the mechanism and leaves out the losses.
Why do the research-chemical sellers rank below the supervised providers on this list? Because “for research use only” or “not for human consumption” is the entire legal basis these products exist under. No regulator has checked them for identity, strength, or purity, and without independent batch-level testing there’s no way to know which vendor’s vial is actually cleaner. Layer that uncertainty on the failed-trial record and you get the gap in the ranking.
What is larazotide and what does it actually do in the body?
Larazotide is a short synthetic peptide built to tighten the junctions between intestinal cells, the microscopic doors that decide what crosses from your gut into your bloodstream. The theory is that lowering intestinal permeability (what people call leaky gut) might ease symptoms in conditions like celiac disease. It doesn’t break down gluten and it doesn’t stop an immune reaction once it’s underway. It’s aimed at the doors, not the alarm system.
Is larazotide legal to buy, and what is its current regulatory status?
The FDA hasn’t approved larazotide, so no company can legally sell it as a finished medication, over the counter or online. Research-chemical vendors sidestep that by labeling it for research use only, which gets them around pharmaceutical regulation but doesn’t make buying it for personal use a clean transaction. The clean route is a physician-supervised compounding pharmacy like FormBlends, operating under state pharmacy board oversight.
Does larazotide actually work, and how strong is the evidence?
By the numbers above: one primary endpoint met out of four major trials, and that one win only held at the lowest dose tested. The evidence is promising in patches but not conclusive, and the confirmatory Phase 3 trial didn’t pan out. Outside celiac disease, human data is thin to nonexistent. Cell and animal work supports the mechanism, but that’s never been a reliable stand-in for human trial results. Treat the science as early and unsettled, not closed.
What side effects and safety concerns should I know about before using larazotide?
Across the published trials, larazotide was generally well tolerated, with headache and nausea as the most common complaints, and no prominent pattern of serious adverse events. But those trials used pharmaceutical-grade material under medical supervision. That safety record doesn’t automatically transfer to peptides bought from unvetted online sellers, where purity and dosing accuracy can swing widely. Long-term safety data doesn’t exist yet, for anyone.
References
- Phase 2b dose-ranging study (n=86) of larazotide acetate with gluten challenge; the primary endpoint of reducing intestinal permeability (lactulose-to-mannitol ratio) was not met, with results affected by high inter-patient variability, though some symptom measures improved at lower doses. Leffler DA et al., American Journal of Gastroenterology, 2012;107(10):1554-1562. [P1] https://pubmed.ncbi.nlm.nih.gov/22825365/
- Randomized placebo-controlled gluten-challenge study (n=184); larazotide reduced gluten-induced symptoms and immune reactivity, but no significant difference in the lactulose-to-mannitol ratio was observed between larazotide and placebo. Kelly CP et al., Alimentary Pharmacology & Therapeutics, 2013;37(2):252-262. [P2] https://pubmed.ncbi.nlm.nih.gov/23163616/
- Randomized controlled trial (n=342) in adults with persistent symptoms despite a gluten-free diet; the primary endpoint was met with the 0.5 mg dose, while the higher 1 mg and 2 mg doses did not separate from placebo. Leffler DA et al., Gastroenterology, 2015;148(7):1311-1319. [P3]
- The Phase 3 CeDLara trial, the first Phase 3 trial in celiac disease, was discontinued in June 2022 after an interim analysis found the additional patient numbers needed to show a meaningful effect were too large to support continuation; larazotide was not FDA-approved. Celiac Disease Foundation, 2022. [P4]
- Systematic review and meta-analysis of 4 randomized controlled trials (626 patients) concluding larazotide acetate appeared safe and was somewhat superior to placebo in alleviating gastrointestinal symptoms during gluten challenge, while noting it is less likely to offer a definitive cure and that additional trials are warranted. Hoilat GJ et al., Clinical Research in Hepatology and Gastroenterology, 2022;46(1). [P5]
- FDA official lists of bulk drug substances for use in compounding under section 503A; the status of compounded peptides has been shifting. U.S. Food and Drug Administration.
- Independent comparison of where to buy peptides in 2026, supervised telehealth versus the gray market. [R1]
Written by Hassan Sato, independent journalist. Reviewing the trials and labels directly. Last reviewed April 2026.
Not professional medical advice. Speak with your healthcare provider before making a change.





